

Author: Randeep Singh / go to all articles on Yoga Concepts
Awake or asleep, we breathe an average of 12 times a minute. During heavy physical exercise, the breathing rate will increase considerably, up to 80 times a minute.
The purpose of moving so much air in and out of the body is, to enable the lungs to do two things: to extract the oxygen needed to sustain life,and to rid the body of the carbon dioxide, that is, the waste product of internal chemical processes.
Before the air reaches the lungs, however, it passes through a series of filters to purify it. Yes, this is not a totally fail-safe-system, and illnesses can and do result, particularly if people smoke, or work in industries where they are exposed to certain kinds of dust.
Breathing Process – Inhalation and Exhalation
Breathing process two processes i.e., inhaling of air called inspiration and exhaling air called expiration.
Inhaling – Inspiration
As air enters the nose, dust particles and other foreign bodies are trapped by coarse hairs. The air continues its passage into the nasal cavity when the moist membrane that lines the walls warms the air and produces mucous to collect even more particles of dust. Hair like projections on the membrane, called cilia, are continually in motion, pushing the film of mucous and its trapped contents back towards the throat to be swallowed.
At the back of the nasal cavity and above the mouth lies two bodies of lymph glands, the tonsils and the adenoids. Because there role is to pick up and destroy invading bacteria, they often become infected and swollen, causing tonsillitis. A sustained build -up of invading bacteria also creates the swelling and irritation of the throat that causes colds and flu.
From the throat, the filtered, moistened, and the warmed air passes into the wind pipe, the trachea, where, as in the nasal cavity, the cilia waft the mucous layer and its contents towards the throat for disposal by swallowing. Once past the trachea, the inhaled air has received all the screening it will receive before passing into the lungs where oxygen from it is absorbed.
At its lower end, the windpipe divides into two smaller tubes called the bronchi, one leading to each lung. It is here that infections such as those that cause bronchitis and pneumonia can build up and cause severe breathing problems.
Within the lungs, each bronchus divides into smaller tubes, the bronchioles, these in turn branch and form millions of tiny air sacs, the alveoli – each surrounded by a mesh work of fine capillaries – where the exchange of oxygen and carbon dioxide takes place.
The branches of the pulmonary artery carry carbon dioxide rich blood, and this gas is given up in return for the oxygen in the new air which has entered the alveolar sacs. The lungs then exhale the carbon dioxide in the de-oxygenated air, along with a certain amount of water vapor, which comes from the moist membranes of the alveoli.
On the cold days this water vapor condenses and shows up as steaming breath. The lungs fill most of the chest cavity and are inflated and deflated by muscular movements of the chest, and the rise and fall of a sheet of muscle, the diaphragm.
Inspiration is an active process. The thoracic cavity expands due to contraction of muscles. The parietal pleura, which is attached to the chest wall follows the expansion of the chest wall. The visceral pleura also follows the parietal pleura and the lungs are expanded because of attachment of the visceral pleura to the lungs.
This creates a sub-atmospheric pressure in the alveoli and air from the atmosphere is drawn inside the lungs. This is inspiration.
Enlargement of Thoracic Cavity – Inhalation
Enlargement of thoracic cavity during inspiration is brought about by the action of three different sections of the chest area.
Elevation of Ribs
The elevation of ribs can be classified into three components.
- Thoracic lid or Operculum (1st rib and manubrium sterni): Contraction of the scalene muscle moves the first rib upwards to a more horizontal position, and manubrium is drawn up-ward and forward. This causes increase of antero-posterior diameter of thoracic cavity. This movement is very slight during light breathing.
- Upper Coastal Series (2nd to 6th ribs): When the external intercoastal muscle contract, the ribs move upward and assume a horizontal position, and this results in increase of antero-posterior diameter of thorax. This action is similar to the movement of the handle of a pump.
- Lower Coastal Series (7th to 10th rib): The contraction of intercoastal muscle causes movement of lower ribs to swing upward and outward, which leads to increase of transverse diameter. This action is like bucket handle movement.
Descent of Diaphragm
It is the main muscle of inspiration. During relaxation, it becomes dome shaped. During inspiration when it contracts, it becomes straight and descend down. This causes an increase in the vertical diameter of thoracic cage. The range of movement of the diaphragm is about 1.5 cm during normal breathing and 6 -7 cm during deep breathing. The diaphragmatic descent contribute about 7.5 percent of the tidal volume of air.
Accessary Muscles of Inspiration
In normal breathing, their action is negligible, but during forced / controlled breathing, they get activated. The muscles are sternocedomastoid – helps in elevation of sternum, alae masei (muscles of nose), and 9 intrinsic muscles of larynx.
Exhalation, Expiration in Breathing
Expiration, or exhalation in normal breathing is completely a passive process: the diaphragm is drawn up, the intercostal muscles, the ones which pull the ribs upwards and outwards, relax and the natural elasticity of the lung tissue forces the air out, this is exhalation.
Forced expiration occurs during coughing, blowing, exercise, and in bronchial asthma. Forced expiration or difficult breathing expiration require muscle contraction also, therefore, it becomes an active process.
The muscles which are involved in exhalation are :
- Anterior abdominal wall muscles: These abdominal muscles, include abdominal recti, transverse abdominis, internal and external oblique muscles. These muscles contract during forced expiration which pushes the diaphragm upwards and reduces the vertical diameter of thoracic cavity.
- Internal intercoastal muscles: Contraction of internal intercoastal muscles depresses the ribs and reduces the thoracic girth.
- Accessory Muscles : The accessory muscles include pectoralis major, adductor muscles of vocal cords.
Pressure Changes during Breathing Movement
The inflation and deflation of lungs are associated with changes in pulmonary volumes and are necessarily accompanied by pressure changes in the lungs (intrapulmonary pressure) and on the pleural surfaces (intrapleural pressure).
Intrapulmonary Pressure
As the lungs expand during inspiration, the intrapulmonary pressure falls to -3 mm of Hg. As the air enters the lungs, the negative value decreases and at the end of inspiration it becomes zero.
During expiration, the intrapulmonary pressure rises to +3 mm of hg, but at the end of the expiration it is again zero.
Intrapleural Pressure
The pressure inside the pleural cavity (pleura is the thin layer of tissue that envelops the lungs and form the inner lining of the chest cavity) is the intrapleural pressure.
Breathing Mechanism
The normal rate of breathing in an adult is about 14 – 18 breaths per minute with a tidal volume of 500 ml. Breathing is controlled by a special group of nerve cells in the brain stem, medulla oblongata, which constitutes the respiratory center of the brain, and is regulated according to the levels of carbon dioxide in the blood, rather than the amount of oxygen present.
The brain will respond to an increased production of carbon dioxide, such as when the body undergoes physical exercise, and adjust the breathing rate accordingly. Holding your breath either deliberately – when swimming under water or practicing pranayama) or unwittingly as a result of an attack of nerves – also alters the breathing pattern.
The carbon dioxide level falls after the first few deep breaths, which are then held, and the brain ceases to be stimulated. This can lead to a blackout and, when swimming under water, death by drowning if the person cannot return to the surface.
Respiratory Centre – Breathing
The respiratory center is a widely dispersed group of neurons located bilaterally in the reticular substance of the medulla oblongata and pons. Respiratory center is divided into three areas:
- A dorsal medullary group of neurons which is mainly an inspiratory area.
- A ventral respiratory group of neurons which is mainly an expiratory area.
- An area in the pons that helps to control the respiratory rate, called the pneumotaxic area.
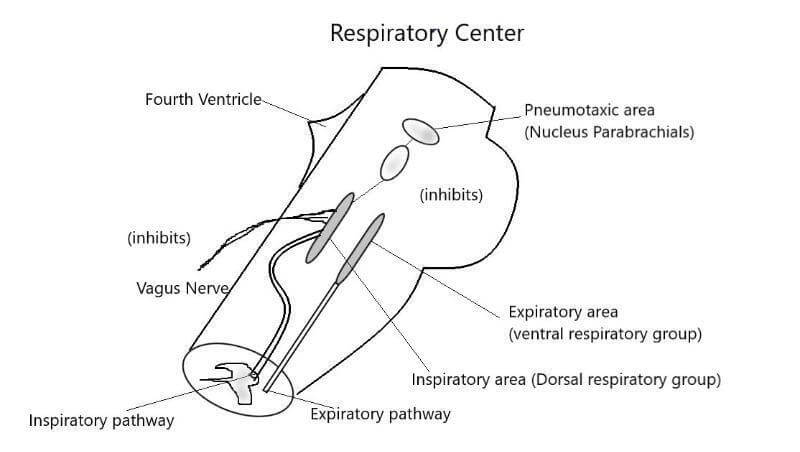
Inspiratory Area
The inspiratory area lies bilaterally in the dorsal portion of the medulla extending approximately along the entire length of the medulla. The inspiratory area plays the fundamental role in the control of inspiration. The basic rhythm of breathing is generated in the inspiratory area.
During inspiration, the inspiratory center becomes dormant, but after a few seconds, the inspiratory area suddenly and automatically turns on again. During the next few seconds the intensity of inspiratory signals increases rapidly, causing the diaphragm and other inspiratory muscles to contract more and more forcefully.
In normal breathing this ‘ramp’ increase in inspiratory signals lasts for about 2 seconds and at the end of which it suddenly comes to a halt. Then the inspiratory neurons remain dormant again for approximately 3 seconds before the beginning of the new cycle again
Expiratory Area
The expiratory are lies bilaterally in the medulla. The expiratory area remain dormant during normal breathing, because expiration results from passive recoil of the lungs and thoracic cavity. During deep breathing, when the pulmonary ventilation becomes greater than normal, signals enter the expiratory area from the inspiratory area.
This stimulation excites the expiratory muscles which contribute the contractile forces to the pulmonary ventilatory process.
Pneumotaxic Area
The pneumotaxic area center is located in the pons. it transmits impulses continuously to the inspiratory area. The main effect is that it stops the inspiratory signal just before the lungs become over inflated. When inspiratory signal stops, expiration occurs. Thus, the main function of the pneumotaxic area is to limit the inspiration which helps to control the respiratory rate.
Apneustic Area
This center is located in the lower part of the pons. It transmits signal into the inspiratory area to prevent the turning off of the inspiratory ramp signal.
Factors influencing the Breathing (respiratory) Center
The respiratory center is controlled by many factors which can be classified under two heading: Nervous factors and Chemical factors.
Nervous Factors
Cerebral Cortex
- Stimulation of cingulate gyrus or ventral surface of frontal cortex will inhibit breathing.
- Stimulation of motor cortex stimulate breathing.
Hypothalamus and Lymbic System
- Pain and emotional disturbances (fear, anger, anxiety) stimulate respiration.
- Fever acts via anterior hypothalamus produces rapid and shallow respiration.
Hering Breuer demonstrated that inflation of the lungs inhibits inspiration and initiates expiration, while the deflation of lungs inhibits expiration and evoke inspiratory activity. The two components are called Hering-Breuer inflation and deflation reflexes respectively/
Hering-Breuer Inflation reflex
The receptors for these reflexes are “stretch receptors” located in the lungs, bronchi, and bronchioles. The are stimulated during inspiration. The afferent impulses travel in the vagi and are relayed in ‘tractus solitarius” before they reach the respiratory – inhibitory effect. The inspiration is thus cut off in time and expiration commences
Inspiration – inflation of lungs – stretch receptors stimulated – impulse generated and carried through vagal (efferent) nerve fibers – respiratory center – inhibition of inspiratory center – expiration starts
Recent evidence indicates that Hering-Breuer reflex does not function during normal breathing and in infants. It is active only during deep breathing.
Hering-Breuer Deflation Reflex
If the lungs are extremely deflated, impulses are set up in another type of receptors, which travel up via Vagus nerve to stimulate inspiration. This reflex is not present during normal breathing but comes into action in conditions like Pneumothorax, Hydrothorax where the degree of collapse of lungs is more severe.
J Receptors (Juxta Capillary Receptors)
These are located in alveolar walls close to the pulmonary capillaries and are stimulated by increase in interstitial fluid volume in alveolar walls. They respond to pulmonary congestion, edema, microemboli and to chemicals injected into pulmonary circulation and reflexly produces apnoea, rapid shallow breathing, bradycardia, and hypotension.
Lung Irritant Receptors
This receptor lies between airway epithelial cells in the respiratory tract. These receptors respond to chemical and mechanical irritants (noxious gases, cigarette smoke, dust, cold air) and marked inflation and deflation of lungs. The reflex effect of stimulation of irritant receptors are bronchoconstriction, hyperpnoea, and cough.
Breathing Reflexes from Baroreceptors
The baroreceptors are situated along the collagenous fibers in the walls of the carotid sinus and aortic arch. The carotid sinus is the dilation present at the commencement of internal carotid artery.
A sudden rise in arterial pressure stimulates the baroreceptors and reflexly inhibits breathing, resulting in reduction of rate and depth of breathing. A fall in blood pressure stimulates respiration and increases the rate and depth of breathing.
Chemical Factors which affect Breathing
The two most important chemical factors which affect respiration are:
Carbon Dioxide
When the inspired air carbon dioxide concentration is increased to 2 percent , the pulomanary ventilation increases slightly.
Carbondioxide 4 percent – Pulmonary ventilation doubles.
5 – 10 percent – Pulmonary ventilation increases 8 times.
When inspired carbon dioxide concentration is high, PCO2 (partial pressure of carbon dioxide) is increased. This stimulates breathing, increases pulmonary ventilation and washes out more carbon dioxide from the alveoli, restoring alveolar and arterial PCO2 to normal.
A reduction in alveolar PCO2 inhibits breathing. This diminished pulmonary ventilation results in retention of carbon dioxide which restores alveolar and arterial PCO2.
Mode of action of CO2
Carbon Dioxide stimulates breathing by central chemoreceptors and peripheral chemoreceptors.
Action of carbon dioxide-
- 80 percent by central chemoreceptors – central action on medullary neurons.
- 20 percent by peripheral chemoreceptors – stimulating carotid and aortic bodies.
The central chemoreceptors are present on the ventral surface of medulla.
When carbon dioxide concentration rises, it is converted into carbonic acid, H positive ions liberated – stimulation of chemosensitive area – stimulation of inspiratory area. Increase in hydrogen ion concentration stimulates respiration and increases both the rate and depth of breathing.
A decrease in hydrogen ion concentration depresses breathing and reduces pulmonary ventilation.
Oxygen
The direct affect of lack of oxygen in respiratory center is depression, but normally the depression effect is overcome by powerful chemoreceptor drive and results in hyperventilation.
The overall effect is, lack of oxygen stimulates as well as increases the rate and depth of breathing.
Mechanics of Breathing Disorders
Although subject to many different form of injury, disorders, the lungs have only a few basic ways of reacting. Insults as varied as inhaled toxic gases, drugs, viruses, or lack of oxygen due to shock, trauma or mountain sickness all produce a profound outpouring of fluid into the alveoli (pulmonary oedema) which may effectively drown the patient if untreated.
Bacterial infections cause the alveoli to fill with pus, while chronic bronchitis causes progressive destruction of the bronchial walls. However, all these conditions if not arrested or cured, progress in a similar fashion to destruction of functioning lung tissue and it’s replacement with fibrous scars. This severely impairs the patients ability to transfer oxygen to the blood.
Prevention is therefore very important. You should be aware of toxic materials in your work place and take suitable precautions. Any productive cough that does not clear up in a week or two should be treated by a doctor. Above all, you should not take up smoking or, if already a smoker, you should make every effort to stop, since cigarette smoking is probably the single most destructive factor in causing chronic lung disease.
Breathing Disorders
| Condition | Symptoms | Action |
|---|---|---|
| Common Cold | Running eyes and nose, coughing, sneezing, sore throat, and headache | Colds rarely last for more than a week, but if they persist, can lead to complications such a bronchitis. There is no known cure but aspirin or antihistamine may make the symptoms less uncomfortable. Keep warm and stay indoors. Antibiotics will not help but a lot of whisky may. |
| Tonsilitis | Chills, high fever, pain in tonsil area, difficulty swallowing, headache, pain in jaw and neck. Tonsils red, enlarged, spotted. | Antibiotic or sulphonamide drugs, cold drinks or ice cream. Seek medical attention: if severe or untreated, can lead to other diseases such as rheumatic fever. |
| Acute Bronchitis | Dry, irritating cough with thick yellow mucus and light fever, Cough persists for up to two weeks. | Bed rest in a humid room with inhalants, plenty of hot drinks, Stimulant cough medicine by day and a sedative linctus by night. |
| Chronic Bronchitis | Constant vigorous cough that is worse in the mornings than the evenings. Coughing a clear sputum that may become yellow if a secondary infection sets in. | Antibiotics to prevent secondary infection, breathing exercises, clean air and no smoking. Immediate treatment of all other respiratory ailments. |
| Asthma | Shortness of breath, difficulty in breathing, tight chest, wheezing, sweating. | Test for allergies or infection. Treat with appropriate drugs. Breathing exercises and bronchodilators also give relief. Avoid stressful situations and catching colds or other breathing infections. Prolonged attacks require hospitalization. |
| Pleurisy | Pain caused by coughing, breathing heavily, or moving. The pain may occur in the shoulder, for example, if the pleura covering the diaphragm is affected. | Pleurisy is almost always caused by a virus or bacterial infection and is often associated with pneumonia. Painkillers relieve the discomfort, and appropriate treatment for the particular infection should be prescribed. |
| Pneumonia | Sudden fever, chest pain, cough and blood stained sputum, sweating, shivering, and often vomiting, and diarrhea. | Bed rest, antibiotics and breathing exercises under the doctor’s supervision. |
| Tuberculosis | Children: Fever, swollen lymph glands in the chest, weight loss, coughing, and breathlessness. Adults: Fever, heavy sweating at night, fatigue, weight loss, coughing, blood tinged sputum, and possible pleurisy. | Drugs clear up most infections quite quickly. More serious forms require hospital treatment for up to three months and prescribed drugs for up to eighteen months after. |
| Emphysema | Increasing feeling of constriction of the chest and breathlessness. Frequent coughing attacks and production of sputum. | Emphysema is the consequence of breathing ailments like chronic bronchitis and pneumoconiosis. Treatment consists of clean air, no smoking and breathing exercises. Severe cases may need oxygen before physical activity or sleep. |
| Pneumoconiosis | Spitting blood, coughing, and breathlessness. Possibly asthma. | Pneumoconiosis means any lung disease caused by inhaling dust particles. Some dusts are harmless, but silica and asbestos cause damage to the lung tissue and early treatment is essential. |
| Lung Cancer | Coughing with sputum that may be blood stained. Later pneumonia and partial lung collapse, followed by weakness, weight loss, and lethargy. | Surgical removal of the tumor is possible, radiotherapy and drug therapy are the usual treatments. |
| Laryngotracheo-bronchitis (grou) | Sudden onset of high fever, followed by croupy, non-productive cough, then thick phlegm in the bronchi and trachea, extreme shortness of breath. | If in a child, urgent medical attention advised. Antibiotics given; sometimes hospitalization is necessary. At home, keep room warm, take prescribed drugs. |
Read other Informative Articles….
Basics of Emotions and Feelings
Yoga Sutra 12 Chapter 1 – Abhyasa and Vairagya